




A scientific study has confirmed what many cannabis critics have been claiming for a long time: Cannabis can trigger depression, but this only applies to people with a genetic predisposition. The question that remains unanswered is whether cannabis can treat depression in those that lack the genetic predisposition but still suffer from depression.
Although nowadays, we know of many medical complaints that are potentially treated by the healing effects of cannabis, there are conditions and illnesses where the benefits are not so obvious.
Similarly, while the risks relating to the use of cannabis are clearly defined for some psychological illnesses, for others they are largely unknown. Of all these potential areas, where scientific knowledge of the potential effects of cannabis use on mental health is still relatively unclear, it is probably its relationship to depression where the least is known.
We do know that endocannabinoids influence our moods. However, it has not yet been discovered whether human consumption of cannabis by people who suffer from depression improves or worsens their emotional state, or has no effect at all.
The situation is similar for other mental illnesses. Many different studies have been carried out to try and prove the causal relationship between use of cannabis and the appearance of other psychiatric conditions, such as schizophrenia. Cannabis use is likely to increase the risk of developing schizophrenia and other psychoses; the higher the use, the greater the risk.

There is moderate evidence of a statistical association between cannabis use and a small increased risk for the development of depressive disorders. Anecdotal reports tell us, however, that you should not generalise. There are people who benefit from cannabis and others for whom it is not suitable. There is always someone who has a friend whose deep depression was cured by smoking cannabis, and someone else who knows someone who was able to stop taking his medication by starting to smoke joints.
On the other hand, people have friends who became depressed from consuming cannabis. In fact, examples can be found for all possible arguments. Everyone is probably a little bit right. It is highly likely that these anecdotal reports reflect the reality of the relationship between cannabis and depression more accurately than is the case for other conditions where the connections are less clear.
The links between cannabis use and depressive symptoms are conditional on the individual’s genetic makeup. This, at least, seems to be the conclusion of a study, that was published in the well-known scientific journal Addiction Biology by R. Otten and RC. Engels. But before we look at it more closely, we should briefly define what is meant by a depression.
A widespread disease: depression
Depression is one of the most significant health issues of the modern world. According to the World Health Organization (WHO), there are now 300 million people around the world who are affected by depression. The disease affects people of both sexes, across all age groups and under totally different circumstances.
The symptoms include a depressed mood, loss of interest or pleasure in daily activities, feelings of guilt or low self-esteem, difficult in concentrating, disturbed sleep or loss of appetite and low energy. Depression can lead to suicide, a tragic cause of death that costs hundreds of thousands of human lives each year.
Classification of Otten and Engels’ study
Let us start by saying: The study referred to above was not planned in order to determine how the use of cannabis could be suitable for treatment of depression, but rather to look at discovering whether there is any link between cannabis consumption and the start of depressive symptoms.
The results did not find conclusive support for the idea that depressive symptoms affect cannabis use.
This is a long-term study involving a group of 310 young people who were monitored for four years. Every year, the participants had to take part in a series of tests used to evaluate indicators of depression. A genetic analysis was also carried out on the young people to see to what extent they had a genetic predisposition to depression.
The importance of individual sensitivities
As with all psychiatric illnesses, there are many very different reasons for depression. Although the relationship between the genetic predisposition and the stresses of environmental factors can influence the nature of the disorder, there are no purely genetic and no purely socially triggered mental illnesses.
Rather, you can assume that a specific genetic variant will make a given individual more susceptible to the development of a mental illness when they are exposed to an environment that will promote the swift development of this condition. It is indeed possible for a genetic predisposition to exist, but for the person to never suffer from any illness, if they do not experience any circumstances that would trigger it.
On the other hand, constant and extreme stress from a damaging environment can trigger a condition even if there was only a very minor genetic predisposition. For example, it is possible that someone who is predisposed genetically to develop schizophrenia, does not develop it, because he is not exposed to circumstances that cause stress and act as triggers. Equally, someone without this genetic predisposition may develop a mental illness due to a traumatic event, such as war traumas.
The biological marker for susceptibility to depression is a gene that encodes the presence of serotonin transporters in the brain. The serotonin transporter is a protein that is responsible for regulating the amount of serotonin present in the nervous system. You can think of this as being a little like a priming pump, that transfers serotonin from outside a neuron to inside it, and so restores balance. The brain perceives this as a positive mood. A certain gene encodes this protein, or rather its activation, so that serotonin receptor protein is produced.
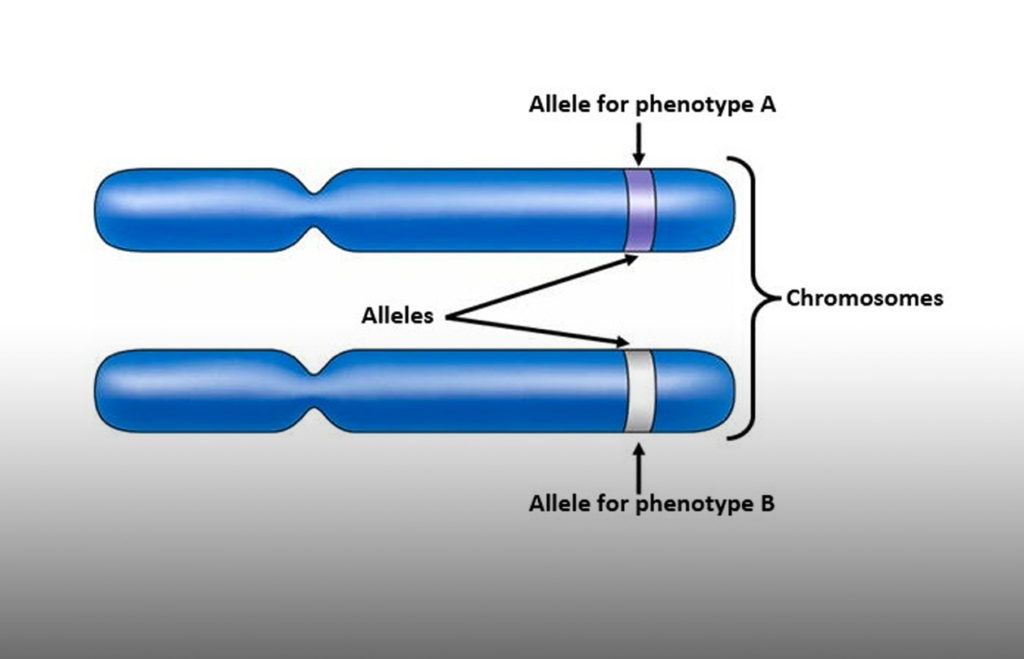
Each gene has two alleles. If this particular gene has “long” alleles (made up of more bases than those of the short allele) then it encodes more serotonin transporters. But if it has “short” alleles (so less bases) then it encodes fewer. It seems that people with a short allele have a greater predisposition to major depressive disorder (in those who have experienced traumatic or stressful life events) than those with a long allele.
Cannabis can trigger depression
But back to Otten and Engels’ study. The researchers tracked children from 428 subject families and carried out various tests on them, to classify their depression. In this way, they found that for 310 of the young people, the genetic markers for depression were present. In addition, their marijuana consumption was determined.
It was discovered that only people with the short version of the gene that codes the serotonin transporter displayed more symptoms of depression over time than those with the long gene. The people with the short allele of the gene who also smoked cannabis had more frequent symptoms of depression.
In other words, smoking marijuana was revealed as an external circumstance, which triggered depression in people who had a genetic predisposition. This result was beyond doubt, even if the young people with the short allele of the gene initially responded euphorically and also displayed other placebo effects of marijuana. In addition, other environmental factors relating to depression were checked, such as, for example, consumption of tobacco and alcohol, educational level, and socio-economic and personality-related factors.
More research is needed
In summary, this interesting piece of research is the first to provide a reliable connection between cannabis consumption and depression and the symptoms of depression. Although it does not provide an answer to the question of whether marijuana may be a useful form of treatment for depression, it shows that its use can trigger forms of depression. That is obviously the case for people with a genetic predisposition, for whom the smoking cannabis is therefore not recommended. Other people are apparently not affected by these problems.
But some questions still remain. Can using cannabis be useful for people who do not show any genetic predisposition, but are still suffering from depression? Maybe the differences in the effect of marijuana on people with depression, which we referred to at the start of this article, corresponds exactly to the genetic differences between different individuals? These questions will need to wait for further research for answers.
What does not appear very useful is to rush off to your GP to have a genetic analysis carried out to find out your predisposition to depression. In my opinion, it is preferable to monitor your own behaviour and decide whether the consumption of cannabis has a positive or negative effect, or no effect at all, and then respond accordingly.
- Disclaimer:This article is not a substitute for professional medical advice, diagnosis, or treatment. Always consult with your doctor or other licensed medical professional. Do not delay seeking medical advice or disregard medical advice due to something you have read on this website.


Fresh cannabis smoothies are used in Central Asian Countries they call it like “Bhaang” i don`t know how to pronounce this word .
This article assumes the only use of cannabis is as we’ve all come to know it – dried, then smoked, vaporized or eaten. Cannabis used this way is psychoactive, and it’s the preferred way when used as a relaxant and intoxicant (the latter term is a misnomer, since cannabis is not toxic).
Cannabis when used in it’s fresh, undried/unheated and non-decarboxylated form – think picked fresh, then used or immediately frozen – is unparalleled at combating depression. The cannabinoids in fresh flowers are still in the acidic form and besides being non-psychoactive, have different and very pronounced health benefits. Over the last year and a half my friends and I have used fresh cannabis flowers – they typical high-THC varieties along with a high-CBD variety – and there are a list of conditions this way of using it has helped us all.
Typically depression is lifted – the soul-deadening, life-is-crap-no-matter-what cloud that forms too often is quickly lifted over the course of the first week of use (at approx. 7gm/day of fresh flowers in a smoothie). Other things we’ve noticed are blood veins/skin tone improves (capillaries that were showing under the skin no longer appear), often energy is increased, and surprisingly – joint mobility is increased as pain from the joints decreases. I can do a deep knee bend now – something I haven’t been able to do without pain and/or help for 5 years or more.
We started this after watching the YouTube video, “Leaf” – which suggests juicing raw cannabis leaf is good for health. Since nobody grows enough to have a glass of leaf juice every day, and especially knowing that the goodness of this plant is always concentrated in the mature flowers, we took it a step further.
There is no better way to use cannabis for health than to eat mature flowers in their raw, unheated/undried state. A friend had terminal kidney disease – diagnosed by three doctors in two states – and after a few months of fresh cannabis smoothies her kidneys are now fully functional. This is anecdotal – a one-off result – but it’s not a cousin of a friend’s nephew – I know this person, and it’s true.
Bottom line – eat it fresh, harvest directly into your freezer and start drinking the most healthy smoothies you’ll ever have.