




Cystic fibrosis is a severe and debilitating genetic disorder that significantly reduces life expectancy and quality of life in sufferers. Now, evidence is emerging of the endocannabinoid system’s fundamental role in the disorder.
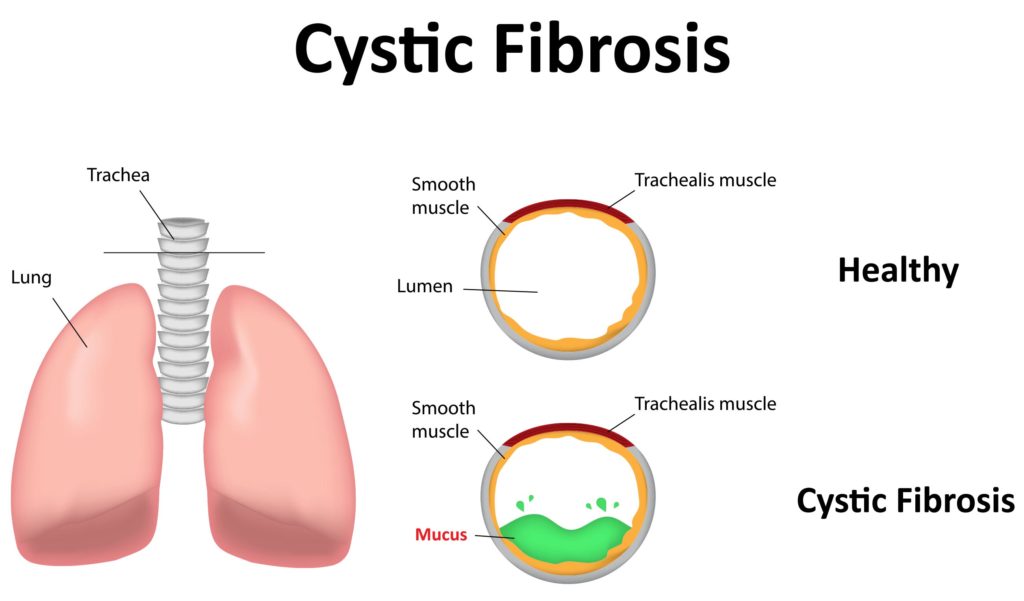
Cystic fibrosis (CF) is a genetic disorder that affects the lungs and various other organs. Symptoms include difficulty breathing and overproduction of sputum as a result of lung infections.
It’s known that CF is associated with a protein known as cystic fibrosis transmembrane conductance regulator (CFTR), the production of which is encoded by the CFTR-gene. People possessing certain single-nucleotide polymorphisms of the CFTR-gene exhibit reduced ability to regulate fluid transport in the epithelial tissues of the lungs, pancreas and various other organs, leading to the development of CF itself.
Now, research is suggesting that this genetic abnormality exerts its effects on the individual via the endocannabinoid system itself.

Fat loss, cystic fibrosis and the endocannabinoid system
Cystic fibrosis (CF) is associated with abnormal lipid metabolism; progressive fat loss is a common symptom of the disease. The lungs and pancreas are most affected, which typically results in progressive lung damage and a condition called “pancreatic insufficiency”. This condition leads to the pancreas being unable to synthesise enzymes in sufficient quantities, resulting in malabsorption of nutrients.
As endocannabinoids are fatty acid derivatives, it’s thought that the imbalanced endocannabinoid system seen in CF sufferers may be a result of this factor.
Due to the potential for malabsorption, sufferers of CF have significantly higher caloric requirements than non-sufferers in order to achieve normal growth and development and maintain good overall health throughout life. Furthermore, researchers have known for some time that in CF, pulmonary health is fundamentally linked to nutritional status; thus, maintaining good dietary health significantly improves long-term prognosis and probability of survival.
Therefore, most CF patients follow a specifically tailored, high-calorie diet in order to achieve normal development and maintain pulmonary health. Diets of CF patients should be carefully controlled and monitored to ensure that adequate nutrition is reaching the patient, and if malnutrition should occur, immediate steps must be taken to reverse it.
In some cases, appetite stimulants can be useful for CF patients suffering from malnutrition, although it’s vital to first ensure the malnutrition is due to insufficient food intake and appetite rather than due to malabsorption. In such cases, treatment with THC could represent an ideal option as it stimulates the appetite.
Related post

Prenatal and postnatal endocannabinoid dysfunction and CF
Recent research has indicated that the development of CF may be associated with dysfunction in the endocannabinoid system during pre- or postnatal development. The endocannabinoid system has a fundamental role to play in various aspects of human development, from the very earliest stages.

High levels of cannabinoid receptors, along with high concentrations of the endocannabinoid anandamide, are present in the newly-formed embryo prior to implantation in the epithelial lining of the uterus; a temporary drop-off in anandamide levels is then necessary to ensure successful implantation of the embryo.
Alongside this, the presence of CB1 receptors in white matter regions of the pre- and postnatal nervous system suggests that these receptors play a specific role in brain development. Furthermore, anandamide has been shown to be present in mother’s milk, and there’s evidence to suggest that activation of CB1 receptors is crucial to the suckling response in newborn mice.
Anandamide has also been shown to exert a neuroprotective effect in the postnatal brain.
Dysfunction at any stage of this process is thought to cause a range of developmental disorders such as CF; potentially, treatment with cannabinoids could mitigate or even reverse such disorders.

How THC administration may lower the risk of CF symptoms developing or worsening
While there have so far been no studies into the potential for cannabinoids to treat human infants with CF, research into mice has yielded promising results.
A 2011 study studied behaviour including motor activity and anxiety levels in mice specifically bred to lack the CFTR gene and exhibit symptoms of CF. Researchers expected to find impairments to the endocannabinoid system in such mice compared to healthy controls.
The researchers predicted that administration of cannabinoid receptor agonists to CF mice during infancy would restore imbalanced cannabinoid levels and prevent behavioural abnormalities. Thus, CF mice treated with THC were compared to wild-type mice and untreated CF mice for anxiety and motor activity levels.
It was demonstrated that CF mice untreated with THC exhibited decreased motor activity and increased anxiety in adulthood compared to wild-type controls, while adult CF mice treated with THC in infancy showed normal motor activity and anxiety.
The researchers suggested that behavioural alterations in CF result primarily from a lack of the CFTR-gene. They hypothesize this causes neural cells to lack an important neurotransmitter signalling system known as the CFTR-channel, and secondarily mediated by fatty acid deficiencies and imbalanced levels of endocannabinoids and their receptors.
They furthermore suggested that intensive treatment with cannabinoids during infancy could restore balance to the endocannabinoid system and mitigate behavioural abnormalities in adulthood.
Easing inflammation in cystic fibrosis lung disease with CBD & THC
CF patients are at great risk of developing lung disease. The inflammation associated with CF lung disease impairs lung function and can lead to respiratory failure, making it one of the leading causes of mortality. Therefore, preventing or easing this inflammation is vital.
Research shows that both THC and CBD are potent anti-inflammatory agents. Even better, they don’t come with the side effects that many of the current CF drugs do. Knowing this, it should be clear that further research and development of cannabinoid-based CF treatments are needed and are likely coming.

Cannabis use by existing cystic fibrosis patients
Although overall substance use in CF patients is lower than in the general population, cannabis is used surprisingly frequently. A 2012 survey published in the Journal of Cystic Fibrosis found that 31% of surveyed CF patients have used cannabis.
A 2001 review stated that there have been “no long-term studies looking at marijuana use in the CF population, but several papers have observed a disturbing prevalence of up to 60%. Some patients may find they obtain transient broncho-dilator effect (sic.) from smoking marijuana, but this benefit is very short-lived and patients need to be aware of the long-term damage from both the tobacco products and the metabolites of the marijuana”.
An earlier study found that cannabis “often aggravated chronic pulmonary symptoms, although some patients reported transient relief during use”.
Of course, this review assumes that cannabis is smoked alongside tobacco, and is specifically discussing the dangers of smoking cannabis rather than other forms of consumption. While recent studies have suggested that cannabis smoke is less carcinogenic than tobacco smoke, it’s not recommended for people who are prone to lung issues to smoke anything. Until more is known about the health risks of smoking pure cannabis, patients will usually be advised by their doctor to opt for healthier consumption methods, such as vaporizing and edibles.
Related post

Implications for healthcare
Much research remains to be done before we’ll have gained a complete understanding of the intricacies of the endocannabinoid system, its importance to human development, and its relationship to many previously mysterious diseases such as cystic fibrosis. However, initial research into the importance of cannabinoid receptor agonists such as THC is highly promising, and no doubt will provide the basis for future targeted therapies.
- Disclaimer:This article is not a substitute for professional medical advice, diagnosis, or treatment. Always consult with your doctor or other licensed medical professional. Do not delay seeking medical advice or disregard medical advice due to something you have read on this website.


What if, because people with cystic fibrosis have a impaired ability to metabolize lipids/fats, and one must be able to metabolize fats to allow good synthesis or creation of anandamide and 2-AG and the THC in the cannabis is supplementing them with as a substitute for Anandamide and 2-AG? If this is true, then the ramifications are huge. And it could explain the higher than average practice of those with cystic fibrosis “abusing” cannabis? Maybe it could save their lives? I don’t know this answer yet, but I certainly think we need to explore it. Thank you for asking a good question.
I have looked deeper and it is more complex, but still a very intriguing question.
i really enjoyed reading this article and the other people leaving comments are all haters. ive had CF for 21 years and smoking strictly tree for 7years and IT DOES HELP in every shape and form. I look forward to reading other studies involving marijuana and CF patients in the future!
This is completely incoherent. CF doesn’t develop. The condition and the associated symptoms can change, worsen or evolve over time but it’s a genetic condition, it’s either there or it’s not. Also you said the THC helped the mice with anxiety and behavioral problems, but what does that have to do with CF? And smoking is LITERALLY the WORST thing someone with CF can do, that being said edibles and vaporizing are still valid options but you didn’t really stress that. Yes CTFR has the letters C and F in it but other than that doesn’t seem like they’re related. Maybe take a smaller bong rip before writing your next piece.
Hello,
After receiving feedback on your comment from the author of this article, the subheading about “CF developing” has been updated to specify “CF symptoms worsening and developing”, as this seems to be the thrust of your complaint. The first and second paragraphs of the article clearly state that CF is a genetic disorder; as quoted below, this use of “development” refers to the genetic level, not the life of the individual sufferer. As you say above, “the associated symptoms can change, worsen or evolve over time”; another way to describe this would be “develop”, so I believe your complaint is more about semantics than facts.
Regarding your question about the experiment with mice, the author does not “blame” the CFTR gene for anxiety. The author merely reports on a study that investigated the effects of THC on anxiety and motor activity in CF mice compared to non-CF mice. If you feel that this is an unfair comparison, we would advise that you take it up with the authors of the study, not the journalist that is merely reporting on the research to date.
Regarding your question about the relation of CF to CTFR (I believe you mean CFTR), which stands for “cystic fibrosis transmembrane conductance regulator”, this paragraph explains the connection: “It is known that CF is associated with a protein known as cystic fibrosis transmembrane conductance regulator (CFTR), the production of which is encoded by the CFTR-gene. Individuals possessing certain single-nucleotide polymorphisms of the CFTR-gene exhibit reduced ability to regulate fluid transport in the epithelial tissues of the lungs, pancreas and various other organs, leading to the development of CF itself.”
I hope this clears up any confusion the article my have caused, and thank you for your feedback.
With best wishes,
Scarlet
one doesn’t develop c.f. it’s in the dan at conception which ,to me, makes this whole article null and void
Hi Joann,
After receiving feedback from the author of this article, the subheading about “CF developing” has been updated to specify “CF symptoms worsening and developing”. The first and second paragraphs of the article clearly state that CF is a genetic disorder; the use of the word “development” here is in reference to the effects of the CFTR-gene and CFTR protein on CF, and describes the action at a genetic level. It is unfortunate that this question of semantics has caused you to disregard the whole article.
I hope this clears up any confusion the article my have caused, and thank you for your feedback.
With best wishes,
Scarlet
This is a ridiculous article which blames cftr gene for anxiety in an effort to link CF to Marijuanna. What a waste of my time.
Hello,
Thank you for your comment. To clarify, the author does not “blame” the CFTR gene for anxiety. The author merely reports on a study that investigated the effects of THC on anxiety and motor activity in CF mice compared to non-CF mice. If you feel that this is an unfair comparison, we would advise that you take it up with the authors of the study, not the journalist that is merely reporting on the research to date.
With best wishes,
Scarlet