




There is mounting evidence for the role of cannabinoids in the treatment of neurodegenerative disorders, traumatic brain injury and ischemic stroke. Aside from having been established as antioxidative and anti-inflammatory, cannabinoids also exhibit neuroprotective qualities. Cannabinoids may even promote neurogenesis.
For the neuroprotective effects of cannabis, the main medical application is in neurodegenerative diseases. Neurodegenerative diseases occur as a result of progressive loss of the function of neurons. The second most common neurodegenerative disease with adult onset is Parkinson’s Disease, with one of the most common being Alzheimer’s. Although neurodegenerative disorders are less prevalent in children, they do exist, most commonly as encephalopathy.
For many neurodegenerative diseases, inflammation and immune response in general is one of the primary factors causing damage and dysfunction of neurons. This is also why many neurodegenerative disorders occur with adult onset.
Currently, there are no treatments to cure neurodegenerative diseases. At most, drugs can mask symptoms and perhaps halt further progression of the disease. This is where the neuroprotective effects of cannabis may have a role to play in neurology.
The endocannabinoid system and neurodegenerative conditions
Scientific research into the endocannabinoid system is revealing more and more about its role in neuroprotection and neurodegenerative diseases. The endocannabinoid system is an extremely complex physiological signalling system, mainly concentrated in the brain. What makes this particular human mechanism so interesting is that it is a signalling system that works in reverse.
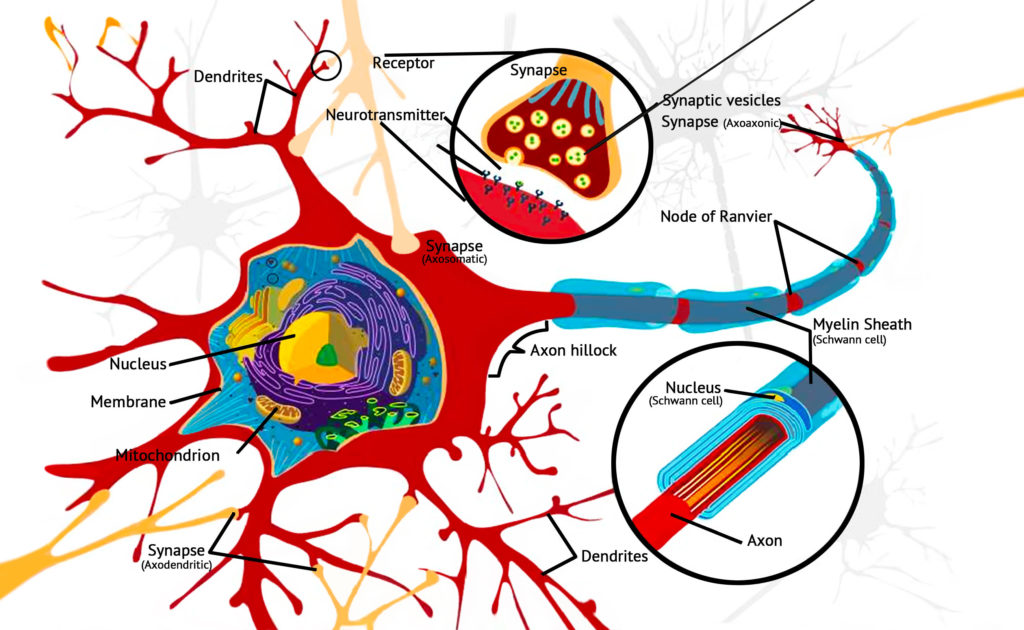
Endogenous cannabinoids are not stored in presynaptic neurons the same way as neurotransmitters. They are produced on demand when the trigger for intracellular synthesis is “switched on”, the main trigger being calcium ions. This is one hypothesis behind why the endocannabinoid system behaves as a “restoration” system or “healing” mechanism of the body.
A relevant example of this is in endocannabinoid levels following brain injury. A 2006 review demonstrated extremely elevated levels of endogenous cannabinoids following kainic-acid induced seizures, glutamate toxicity, shock-induced stress and trauma. The response of the endocannabinoid system to these events suggests that one of the brain’s main compensatory mechanisms following brain injury is endocannabinoid signalling.
These findings show aa possible association between the endocannabinoid system and recovery from neurodegeneration. Cannabis therefore proposes a potential medical target.
Related post

Antioxidative & anti-inflammatory properties of cannabis
In recent years the evidence for the antioxidative and anti-inflammatory properties of various cannabinoids have become well established, and our understanding of the role they play in modulating neurotransmission has grown.
Thus, serious consideration is now being given to their potential as neuroprotective agents. Cannabinoids have been shown to prevent neuronal death in acute neuronal injury, including ischemic stroke and traumatic brain injury, as well as provide symptomatic relief in multiple sclerosis, Huntington’s disease, and other chronic neurodegenerative diseases.
Antioxidant effects are a proposed mechanism of action by which cannabis may provide relief from the symptoms associated with neurodegenerative conditions. As long ago as 1998, researchers demonstrated the antioxidant effects of CBD, noting that it is more potent an antioxidant than ascorbate or tocopherol. An additional benefit is that CBD lacks the toxicity associated with tocopherol.
This is pertinent because the brain is one of the most vulnerable organs to oxidative stress. Oxidative stress is essentially an imbalance in redox states, causing an excessive amount of reactive oxygen species. It has been hypothesized that oxidative stress is a crucial factor in the onset of Alzheimer’s. The same has been suggested for Parkinson’s Disease.
Anti-inflammatory properties of cannabis may also be considered a neuroprotective quality of the plant. It is thought that CB2 receptor-mediated activity that affects microglial cells reduces neuro-inflammatory mechanisms. In the current context of treating neurodegenerative conditions, anti-inflammatory drugs are sometimes used, especially in the treatment of Alzheimer’s. However, so far, very mixed results have been obtained from studies about the efficacy of anti-inflammatories used for this purpose.
Inhibition of damage-causing compounds
A study published in 2002 by Mechoulam et al. demonstrated that production of anandamide and 2-AG increased in the brain following traumatic brain injury. In the event of traumatic brain injury (TBI, or intracranial injury), certain substances are produced that are known to cause neuronal damage: tumour necrosis factor-a and reactive oxygen species (ROS). The study showed that the production of anandamide and 2-AG inhibited the production of these potentially damaging substances. Anandamide and 2-AG are endogenous cannabinoids that are produced by the body’s own endocannabinoid system.
Another Mechoulam study explored the inhibitory potential of 2-AG and anandamide in vivo. The study was conducted on mice and rats with TBI. When both compounds were administered to the brain-injured mice and rats, the extent of brain damage was reduced. Reductions in the extent of brain oedema (accumulation of fluid leading to swelling), infarct volume (extent of tissue necrosis), and hippocampal cell death were all noted, along with a generally improved clinical recovery.
The reason that this is relevant to medicinal cannabis is that CBD is now known to increase serum levels of anandamide. Anandamide is broken down by fatty acid amide hydrolase (FAAH), an integral membrane enzyme. Anandamide is delivered to the FAAH enzyme by a fatty acid-binding protein (FABP). FABPs are proteins responsible for the transporation of other molecules. CBD inhibits FABPs, which in turn disrupts the delivery of anandamide to FAAH, therefore increasing serum levels of anandamide. Interestingly, researchers have also demonstrated that non-cannabinoid cannabis compounds also weakly inhibit MAGL, an enzyme responsible for the breakdown of 2-AG.
Related post

Cannabinoids in post-stroke recovery
THC, CBD and various other cannabinoids have been repeatedly studied to evaluate their neuroprotective influence during and following occurrence of ischemic stroke (IS). While there are various studies indicating that cannabis use can increase risk of stroke, it appears that this phenomenon is limited to a small subset of susceptible individuals. In 27% of these cases, reversible cerebral vasoconstriction triggered by cannabinoids use may be a convincing mechanism of stroke. For the majority, cannabinoid therapies appear to have great potential in mitigating inflammation and oxidative stress due to IS.
CBD has been the subject of much investigation as a neuroprotectant for IS. It has been shown to increase cerebral blood flow following IS and thereby aid in mitigating infarct volume. 14 day-repeated treatment with CBD (10 mg/kg) led to tolerance of hypothermia, and to a tolerance of neuroprotective effects. For this reason, it is seen as having greater therapeutic potential than THC in this area of research. CBD has also been shown to reduce inflammation caused by release of interleukin-1, nitric oxide, and tumour necrosis factor-a following IS.
Just as with TBI, much of the damage subsequent to IS is due to oxidative stress, which is caused by the build-up of ROS due to excessive glutamatergic signalling. Both THC and CBD have been shown to be effective antioxidants (as previously demonstrated) that inhibit glutamatergic signalling and thereby reduce the extent of ROS build-up following ischemic stroke. However, CBD again shows greater effectiveness as an antioxidant and therefore has greater therapeutic potential than THC for degenerative conditions.
Glutamate signalling and cannabinoids
Glutamate is the most abundant neurotransmitter in the human brain. It is an excitatory neurotransmitter that plays a role in neural circuits involved with synaptic plasticity. By strengthening or weakening signalling between neurons, glutamate plays a vital role in learning and memory. It is arguably the most important neurotransmitter in the brain, shaping the way an individual retains information and is an important player in long-term potentiation.
High glutamate levels induce neurotoxicity (particularly mediated by the NMDA, AMPA and kainate glutamate receptors) and lead to the formation of secondary damage-causing compounds such as ROS and tumour necrosis factor-a. It is also known that glutamate activity is reduced by the presence of antioxidants. As CBD and THC have been demonstrated as antioxidants, there is a clear basis for further investigation of cannabinoids in this particular area of neurology.
The interactions between various cannabinoids and the glutamatergic signalling system were investigated in a study titled Neuroprotective Antioxidants from Marijuana, published in 2000. In this study, cannabidiol and several other cannabinoids were investigated for their neuroprotective potential in rats in vitro, in neuron cultures exposed to toxic levels of glutamate. CBD exhibited the most superior antioxidant qualities for the prevention of glutamate toxicity.
Cannabinoid receptor-independent mechanism
The authors of Neuroprotective Antioxidants from Marijuana also demonstrated that both THC and CBD increased neuroprotection and reduced NMDA, AMPA and kainate receptor neurotoxicities. Furthermore, the level of neuroprotection was not increased by the action of specific cannabinoid receptor antagonists, indicating that the mechanism of action was independent of cannabinoid receptors.
Previous studies had concluded that CB2 receptors play a role in these key cell processes. This forms the basis for the idea that selective agonists of this receptor type may act on “two sides of a coin” by providing cytoprotection of healthy neural cells, or by eliciting apoptosis of tumoral cells. However, CBD does not typically behave as an agonist, so its neuroprotective potential must therefore be realised elsewhere.
CBD was also shown to reduce hydroperoxide (a type of ROS) toxicity in neuron cell cultures, further proving its effectiveness as an antioxidant. Although these tests were performed in vitro, preliminary in vivo studies into cerebral ischemia in rats suggest that it is effective across the board.
Related post

Perinatal hypoxic-ischemic event
A significant cause of brain injury in the neonatal period is perinatal hypoxic-ischemic event. This is when the flow of oxygen and blood to the infant brain is interrupted due to asphyxia, often during childbirth. This devastating condition leads to the death of 15-20% of children diagnosed.
This condition can also lead to severe neurological impairment such as epilepsy, cerebral palsy, motor dysfunction and hyperactivity in a further 25%. The developing brain is far more susceptible to hypoxic-ischemic events than the adult brain. Because it contains a high concentration of blood vessels and higher water content, the potential for damage-inducing events such as haemorrhage is greater.
Immediately following hypoxic-ischemic brain injury, a set of specific cellular mechanisms including increased production of glutamate is set in motion, triggering cell damage and finally leading to excitotoxicity (a type of cell death caused by excessive glutamatergic signalling).
The precise nature of this process is not yet fully understood due to the complexity of the molecular mechanisms that underlie the condition. As such, there is a paucity of effective treatment options to mitigate the extent of neuronal damage. Now, however, rapid advances in our understanding of the field have led to a new class of neuroprotective therapies to be assessed and implemented if proven to be effective.
Among them, the endocannabinoid system is under investigation in order to ascertain its specific role in providing neuroprotection to the developing brain. While use of cannabinoid therapies on children remains controversial, there have been sufficient successes with using cannabinoids in various paediatric conditions (including epilepsy and cancer) without detrimental side-effects. As a result, the controversy is now rapidly being replaced with consensus among the scientific community that such therapies may have an application.
Cannabinoids have been proposed as good candidates for the treatment of perinatal brain injuries. As well as modulating neural responses, cannabinoids have been shown to modulate vasodilation due to endothelial cell function and endothelin activity, regulate calcium homeostasis, and possess significant anti-excitotoxic and anti-inflammatory effects.
There is also an indication that cannabinoids may have beneficial effects on white matter. This is brain tissue composed of nerve fibers. In this study, the administration of the selective CB1R agonist ACEA during the early postnatal period (P1 to P14) increases the generation of oligodendrocyte progenitors. WIN, another synthetic cannabinoid, promoted myelination of subcortical white matter in the same study.

Research also points towards the endocannabinoid’s potential as an endogenous repairing response for neurons. CB receptor agonists such as THC may be able to stimulate this endogenous response.
THC’s neuroprotective qualities for the ageing population
A study published in Nature Medicine in 2017 gained a lot of media attention for its somewhat unusual claim that THC may have rejuvenating effects on the ageing brain. Even Forbes and The Guardian published articles about this study.
To carry out the clinical trial called “A chronic low dose of Δ9-tetrahydrocannabinol (THC) restores cognitive function in old mice”, the researchers administered low doses of THC to mice of various ages: 2, 12 and 18 months. In other words, young, mature and old mice. This was carried out regularly over four weeks. The dosage size is significant due to the fact such small doses do not have psychoactive effects such as those resulting from the amounts consumed for recreational use, which are usually greater.
During the period of one month, the team led by Andreas Zimmer evaluated mice’s ability to carry out cognitive tasks such as water maze tests. The team observed the mice’s abilities to recall the location of safe spots or recognise other subjects of the same species that they were exposed to previously.
Curiously, young mice that had not been given low and regular doses of THC performed better in the behavioural tests for memory and learning than young mice who were given regular THC doses. On the other hand, the opposite was the case with older mice: the ones that had received low and regular doses of THC had better results in the tests than mature and old mice that were not administered THC. Mice with regular small doses also performed in a shorter period of time.
This study supports findings that were made previously using synthetic cannabinoid, WIN, where older mice demonstrated improved memory after cannabinoid administration. In the 2018 study, old female mice aged 24 months were injected once with .002mg/kg THC. Compared to vehicle-treated (the vehicle contained mostly saline, and also some ethanol and cremophor) mice, the THC-treated mice performed better on a battery of 6 different behavioural tests. The single injection of THC also increased the level of Sirtuin1, an enzyme linked with neuroplasticity and neuroprotection.
Cognitive decline as a result of aging is not considered a neurodegenerative disease, although it can be considered pathological. There is virtually no treatment for age-related cognitive decline other than maintaining healthy diet, exercise and brain activity. Rodent studies have demonstrated extreme promise for THC specifically in the treatment of cognitive deficits in the aging population, although human studies are required to confirm these results.
A case for cannabinoid acids for neuroprotection
This article has mainly explored phytocannabinoids THC and CBD, but there is also a case for cannabinoids in their acidic form (THC-A and CBD-A). These are the precursors to THC and CBD, and exist before the process of decarboxylation takes place. Decarboxylation removes the carboxylic acid group, therefore turning THC-A into THC (and CBD-A into CBD).

In this 2017 study published in the British Journal of Pharmacology, researchers investigated the potential of six different phytocannabinoids on PPARγ binding. PPARγ is one type of nuclear transcription factor and most commonly has an application in the treatment of diabetes. This is because it regulates responsiveness to insulin in adipose cells. However, the activation of PPARγ also affects microglia, and thus, it has recently piqued interest for its application in chronic neuroinflammatory diseases.
The study found that cannabinoid acids bind and activate with PPARγ much better than their decarboxylated versions. THC-A was found to be neuroprotective in mice, improving motor deficits and preventing striatal degeneration.
The acidic form of THC is non-psychoactive, and is therefore a particularly pertinent medicinal cannabinoid to investigate. Being non-psychoactive, it is appropriate for a wide demographic of people, including children and the elderly, who are the most prone to neurodegenerative conditions.
Related post
Effectiveness of synthetic cannabinoids
As well as endocannabinoids and phytocannabinoids, attention is now being paid to the potential of various synthetic cannabinoids. For example, in a study published in 1999 by the Journal of Neuroscience, the synthetic cannabinoid agonist R(+)-WIN 55212-2 was found to decrease neuron loss in the hippocampus in vivo following global cerebral ischemia in rats. It also reduced infarct volume following focal cerebral ischemia induced by occlusion of the middle cerebral artery.
The less active enantiomer (the “mirror image” molecule), S(-)-WIN 55212-3, was found to be ineffective, and the protective effect of R(+)-WIN 55212-2 was found to be blocked by the action of the CB1 receptor antagonist “N-(piperidin-1-yl)-5-(4-chlorophenyl)-1-(2, 4-dichlorophenyl)-4-methyl-1H-pyrazole-3-carboxamide-HCl”.
Interestingly, R(+)-WIN 55212-2 also protected cultured cerebral cortical neurons from in vitro hypoxia and glucose deprivation, but this effect was insensitive to CB1 and CB2 receptor antagonists. Much further research is needed to ascertain the precise interactions at work here, but it is clear that there are potential applications for this and other synthetic cannabinoids as treatment for cerebral ischemia, including stroke.
Cannabinoids may possess neuroprotective properties
There is abundant evidence in animal models indicating the effectiveness of a whole range of phytocannabinoids, in the management and mitigation of traumatic brain injury, ischemic stroke and age-related cognitive decline. Furthermore, our understanding of the role that the endogenous cannabinoids anandamide and 2-AG play in the modulation of inflammation and cerebral blood flow is growing. This avenue of research makes the endocannabinoid system a target for the treatment of neurodegenerative conditions.
Though much more research is required, especially on human subjects, the body of evidence in support of cannabinoids for the treatment of neurodegenerative disorders continues to grow. The mechanisms of action by which cannabinoids exert neuroprotective properties are widespread, complex and worthy of further investigation.
- Disclaimer:This article is not a substitute for professional medical advice, diagnosis, or treatment. Always consult with your doctor or other licensed medical professional. Do not delay seeking medical advice or disregard medical advice due to something you have read on this website.


Paragraph right before Conclusions: “THCA increases mitochondrial mass.”
Mitochondria are the cells energy manufacturing site. If the mitochondrial mass increases, will cellular metabolism increase? Since tumor cells were used for the experiment, neuroblastoma is a type of tumor, will the tumor grow faster?
Hi Turbot,
This is a really good question, which I’m going to have to consult an expert in order to answer. As we’re heading into the holiday season, please bear with us for a few weeks so that we can provide you with an accurate answer.
With best wishes,
Scarlet
The giant pharmo companies will loose billions if we can all just grow our own medicine for free.
And governments care more about money than people, so untill they find a way to tax it I doubt it will become legal in England, though Scotland and Wales may go for it sooner.
Hi. My brother suffered a hypoxic brain injury last December and is left severely brain damaged. He is 34. And is looking to go home to be cared for by his wife. Hopefully by Xmas. Do you think that cannabis oil or cbd would be beneficial to him as we are hoping to get his meds reduced. But that is very stressful to him. So we are trying to research how this could be beneficial to him. And I’m trying to find sources of information on it please email me a reply of help or links to who can help with advice on this. In the uk
Hi Rhian,
Thank you for commenting, we are sorry to hear about your brother’s condition. As Sensi Seeds is not a medicinal practitioner, I’m afraid we cannot offer any advice on this kind of question other than to consult your GP. We do have this article which is aimed specifically at healthcare professionals who may be unaware of the many properties of cannabis, so when seeing your doctor this might be useful. Also, since you are in the UK I strongly recommend you get in touch with the United Patients Alliance (you can find them on Facebook), a group of people who are campaigning for the acceptance and legalisation of medicinal cannabis, since they also act as a support group and there may be members who are in a similar situation.
With best wishes,
Scarlet
Hi and thank you for your time. I have been involved in the medical cannabis industry since 2008 in Michigan. We are a legal state which leads me to my question. My girlfriend has suffered a blow to the head this summer. She has had head aches, dizziness, and many of the symptoms that accompany the injury. She went to a follow up today because her symptoms are getting worse. The doctors say she may have a blood clot on her brain. I am looking for information that could help. How can we treat the injury topically or ingest it? Any certain strains indica or sativa? Any info about this would help us and many others who the information could benefit. Thank you again for your time.
what a wondrful article. i really didn’t know why i had a bad picture of cannabis and those who use it. We all have that idea that smoking it is irresponsable and reckless, just because we are maybe programmed to think so. the media, the school.. brainwashed us.
i really thank you for this exquisite article that changed this gray opinion of mine. and i will use this sacred plant whenever i feel i need it. fear from cannabis was just inplanted and not scientifically proven.
Hi Rita, I’m thrilled to hear it. As a full-time cannabis writer, hearing that people have been convinced to change their views after reading my work is the best part of the job as it means my efforts are not going to waste.
Yes I have stenosis facit 4and5Disic in spine scoliosis slipped Disc I would love to see something that would help
Hi Jim,
While I have sourced most of the points made in this article, there are a few that I may have missed. I will endeavour to correct this, but if there is a specific point that you wish to view the source for please let me know and I will start there.
Thanks
where’s the sources? where’s the link to studies etc? would appreciate a little update with citing specifc sources.
To whom it may concern
My name is Warren Elliott 57 I,m the single pension and Disable,My friend wrote this because I can,t or spell very much so I dictated what I say I,ve right side Hemiplegia which is my right side is much weaker than the other side threw a car accident 35 years age which left me Brain damage,got arthritis threw out my body, scoliosis in my back, had 22 operation,s ana more to came going to have an operation on my back soon. I can only use one arm to do things which gives me pain all the time.I take pain killers (OxyContin and Endone) I don,t like taking them there very addictive. I smoke which helps much more, when I can get it, afford it. it would be much appreciated if you could help me get Medical Marijuana or Cannabis I,m finding it very expensive MEDICAL trail
Sent from my iPad Australia New South Wales.
Hi Warren,
Unfortunately we are not in a position to assist anybody in obtaining medical cannabis. However, I can perhaps suggest that you may find some support or further information from the community at Nimbin, NSW.
I wish you all the best!
Regards,
Seshata