




Active Tuberculosis (TB) is a debilitating respiratory disease that typically results in death if untreated. Vaccination programs and modern antibiotics have successfully held TB at bay for decades in most developed societies, but new, drug-resistant strains are now emerging. Cannabis has been shown to exert antimicrobial effects on TB and similar microbes.
What is Tuberculosis?
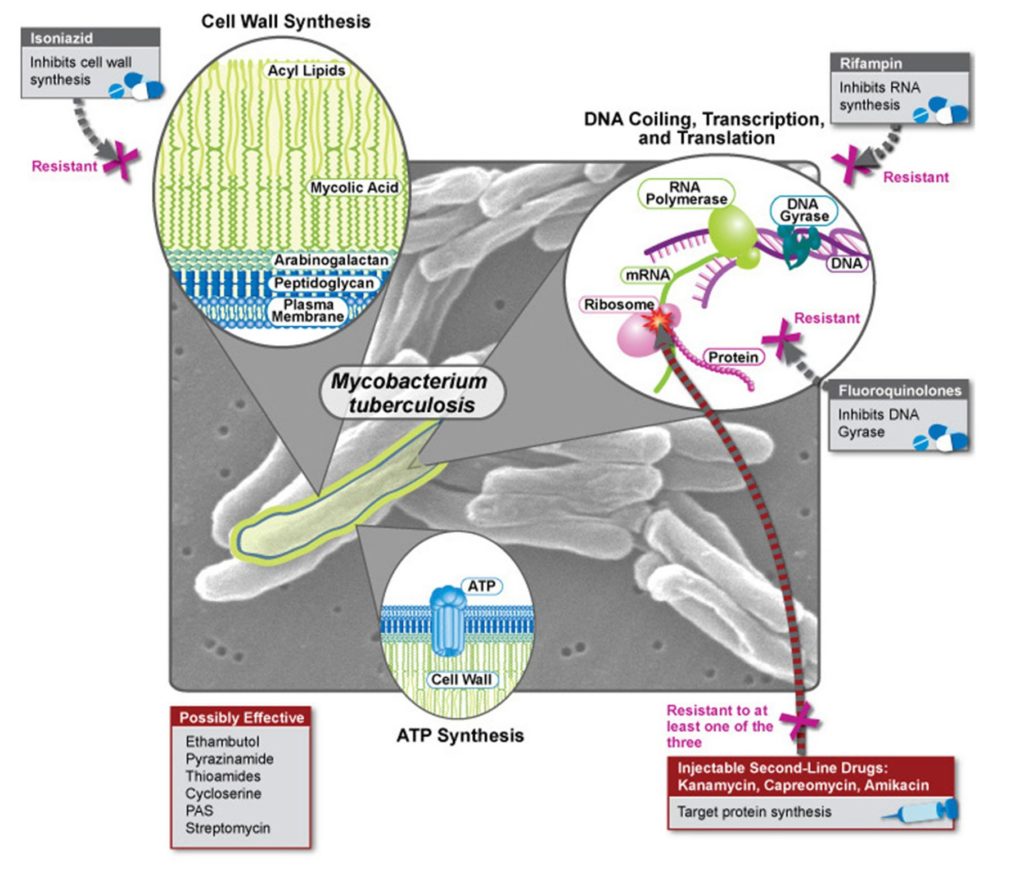
Tuberculosis (also known as TB) is a microbial infection, caused by various strains of mycobacteria (primarily Mycobacterium tuberculosis). Mycobacteria require abundant oxygen to survive and replicate. This is why M. tuberculosis colonises the lungs, and why the leprosy bacterium, M. leprae, forms clusters in the epidermal and epithelial tissues. These tissues receive oxygen from the blood as other tissues do, but can also absorb atmospheric oxygen.
Infection with M. tuberculosis typically leads to a latent (asymptomatic) infection. However, 5-15% of infections lead to an active form of the disease that causes a chronic cough, rapid weight loss, and fever. If left untreated, active tuberculosis has a mortality rate of around 66%. With treatment (usually antibiotics), the likelihood of death is significantly reduced. With that being said, the active disease is difficult and time consuming to treat. This means that the best effort to contain TB rests in prevention and immunisation rather than post-diagnosis treatment.
It is thought that approximately one quarter of the world population has been exposed to M. tuberculosis, with the majority having latent TB infection; around 1% of the world population is infected each year. There were approximately 10 million new TB cases worldwide in 2017 (and 1.3 million deaths from the disease), a 2.6% decrease from 2016. The prevalence and absolute rate of TB is decreasing, and massive gains have been made over the last few decades. However, multi-drug-resistant tuberculosis (MDR-TB) poses a serious and increasing threat.
Drug-resistant tuberculosis
MDR-TB typically occurs when ‘first-line’ antibiotic treatment courses are ceased or interrupted before the bacteria are fully eradicated. In these cases, what remains are often the most resilient forms of the bacterium—those with particularly impermeable cell walls.
MDR-TB can also occur because bacteria cells express genes encoding for drug-modifying enzymes or because cells have mutated entirely. These resilient bacteria then replicate and can be transmitted just as with normal TB. That being said, there is evidence that MDR-TB outbreaks are less likely to arise in healthy populations, and are more common among the immunocompromised, such as HIV/AIDS patients.
Once a TB infection has become multi-drug-resistant, its mortality rate generally increases to around 40%. There are still some drugs that can treat MDR-TB, including some forms of chemotherapy, but the side-effects can be hugely debilitating. If these ‘second-line’ treatments are mismanaged, MDR-TB can become XDR-TB, or extensively-drug-resistant TB. Of all MDR-TB diagnoses, around 10% will progress into XDR-TB. And while XDR-TB is more prevalent in China, India, Russia and South Africa, international travel and migration mean that cases are reported all over the world.
Although MDR-TB is rare and XDR-TB rarer still, it could be disastrous if such strains gain a foothold in the general population. The standard BCG vaccine is not entirely effective against them (or even ‘normal’ TB, against which it is estimated to be approximately 60-80% effective). Thus, new vaccines and treatment options are urgently sought, and governments and international organisations across the planet are pouring money into research and development.
Related post
History of cannabis and TB
A long history of using cannabis to treat tuberculosis has been documented in many parts of the world, and in some cases use of cannabis as a folk treatment for TB has persisted to this day. However, for the most part, the spread of modern medical practices has wiped out cannabis use in folk medicine.
Use of cannabis as a treatment for tuberculosis is first recorded in India, and appears to have been well-known by the time of the Indian Hemp Drugs Commission of 1893-1894. The Commission heard testimony of use of cannabis to treat tuberculosis and a wide range of other conditions, from both Indian and Western doctors, suggesting the practice was also known in contemporary Europe. One unusual custom in India consisted of growing cannabis at the burial site of a killed cobra. The resulting crop was thought to possess exceptional medicinal properties and was particularly prized as a treatment for TB.

Cannabis is an important element of the traditional African pharmacopoeia, and in particular was used by the Zulus of South Africa to treat various illnesses of the respiratory system, including asthma, the common cold, and tuberculosis, which was treated with specially-made decoctions (hot-water infusions). As well as this, there are reports of traditional cannabis use in Mexico as a treatment for tuberculosis.
In this case, sufferers of TB or leprosy (interestingly, given their association) would smoke cannabis heavily to reduce their symptoms. It appears that use in Mexican folk medicine has persisted to the present, although in modern times, tuberculosis is more likely to be treated with an alcohol extract of cannabis. There are also reports of cannabis being used to treat tuberculosis in traditional folk medicine in Argentina.
Hemp seed used to treat tuberculosis in pre-War Czechoslovakia
Extensively-drug-resistant TB is an emerging threat, and new countries are reporting cases every year.
In pre-World War II Czechoslovakia, hemp seed was routinely used as part of a treatment program for children suffering from TB. Prior to 1948 (at which point the Czechoslovakian Pharmaceutical Industry was nationalised) a product called Edezyme was available on the market. Even now, a similar recipe is apparently still produced as a home remedy in some areas.
Ground hemp seed is steeped in warm milk (60-80°C) for at least thirty minutes, before being pressed and filtered. Then, the mixture is administered to the patient on alternate days. Each dose should consist of approximately 375ml of milk and contain 50-80 grams of seed.
Observations recorded over almost thirty years at the Jince Sanatorium in western Czechoslovakia (now part of the Czech Republic) indicated that treatment with hemp seed milk typically resulted in significant improvements, and many successful cures, even in the absence of other medication.
It is thought that the high content of polyunsaturated essential fatty acids found in the primary hemp seed protein, edestin, is important in the treatment of TB. It has been shown that M. tuberculosis bacteria are destroyed at faster rates when high levels of arachidonic acid are present. Arachidonic acid is produced in the body via the metabolism of linoleic acid, which is found in very high levels in hemp seed.
Related post

Modern research into cannabis and TB
In the 1950s, research began to provide evidence of the significant antimicrobial properties of cannabis, and investigations into its potential use as a treatment for tuberculosis began in earnest, with promising initial results. In 1960, it was demonstrated that isolated cannabis resin inhibited growth of M. tuberculosis and various other bacterial pathogens even at dilutions of 1:150,000.
Knowledge of the specific cannabinoids themselves was in its infancy (CBD and CBN had been isolated in the 1940s, but THC and other cannabinoids would not be identified until 1964), and as the world began to strengthen anti-cannabis laws in the 1960s and 1970s, research began to stagnate. However, CBD had been shown to exert specific antimicrobial properties, and as the speed of research began to pick up once more in the 1990s, renewed attention was paid to this area of investigation.
Now, research into the microbial properties of cannabis has uncovered substantial evidence that strains of drug-resistant pneumonia and MRSA are destroyed by several cannabinoids, including CBC, CBG, CBD and THC. In A 2011 Israeli study, rats were injected with M. tuberculosis in order to cause experimental autoimmune encephalomyelitis (an animal model of multiple sclerosis).
The findings showed that subsequent treatment with CBD greatly slowed the progression of TB. The researchers concluded that this effect was mediated by CBD-induced inhibition of T-cell proliferation, a property CBD has also been demonstrated elsewhere to possess. It does not explicitly mention a direct bactericidal effect on M. tuberculosis, but it is possible that it played some role in slowing the progression of the tuberculosis.
Can cannabis use worsen, or even cause TB?
There is substantial evidence demonstrating the link between tobacco smoking and increased risk of tuberculosis infection, which has led some to surmise that cannabis smoking also carries an increased risk. However, there is no evidence to suggest that smoking cannabis (or utilising alternative means of inhaling cannabinoids, such as vaporizing) directly increases the risk of developing tuberculosis.

On the other hand, there is significant evidence demonstrating that the spread of tuberculosis and other contagious respiratory diseases can be facilitated by unsafe methods of consuming cannabis—shared bongs, shared joints, even ‘hot-boxing’ a car or room can increase the chance of tuberculosis microbes being transmitted. In the case of shared bong usage, the risk of transmission may be more than doubled.
Evidence that shared cannabis smoking increases TB risk
In 2003, a cluster of TB cases were recorded in Queensland, Australia, in a group of young Caucasian males (an unusual demographic for the disease—infection rates are typically higher in Aboriginals because prior to European invasion, they had not encountered the disease and had developed no natural resistance). Upon further investigation, members of a close-knit social group were found to be sharing bongs among themselves. The case study concluded that while close household contact was the most significant risk factor, sharing of bongs also significantly increased risk.

In 2004, a group of 11 young tuberculosis patients in Seattle, Washington were found to be linked through social use of cannabis. Of 22 other friends and associates that were subsequently tested, 14 (64%) were found to have positive tuberculin skin test results. Upon investigation, it was discovered that members of the social group regularly shared joints in cars and small rooms (which often had the windows boarded up to conceal illicit cannabis use), and would intentionally ‘hot-box’ their environment. This led to exhaled smoke being repeatedly inhaled, along with whatever microbes were present.
One of the potential issues with identifying cases linked through shared cannabis use is the fact that it remains illegal in much of the world, leading people to be reluctant to name others that may be at risk. This extends the ongoing risk to others outside the immediate social circle, such as co-workers and family members.
For diseases like TB, containing an outbreak before it can become an epidemic is crucial, and this relies primarily on identifying and treating ‘contacts’ of existing cases. This is yet another negative consequence of prohibition, and is, in light of the emergence of new, drug-resistant strains, yet another argument in favour of legalisation, regulation and education.
Related post

Cannabinoids, TB, and the Th1 immune response
When an individual is infected with tuberculosis, a set of immune responses that defines the progression and outcome of the disease is triggered. This immune response differs between individuals, and for the vast majority of humans, no symptoms will ever become apparent. It is not known precisely what mechanisms determine natural immunity to TB. There are multiple different strains, and various different environmental and other factors can exert an influence.
What is known is that the Th1 immune response is vital for defence against intracellular pathogens (microbes that infiltrate and reproduce inside host cells, such as TB), and individuals that are susceptible to symptomatic TB have their Th1 immune response inhibited. In instances of Th1 suppression, the Th2 immune response kicks in. However, this response is designed to defend against extracellular pathogens (such as toxins and parasites), and when forced to attempt to defend against TB, actually allows for more rapid and effective progression of symptoms.
Cannabinoids have been demonstrated to be immune system modulators in several papers. More specifically, it is thought that they inhibit the Th1 immune response while promoting the Th2 response. Thus, in instances where activation of the Th1 immune response is crucial to fighting off an infection, as is the case with tuberculosis, it would appear that avoiding the use of cannabis would be advantageous.
It is clear that much research remains to be done on the complex relationship between the endocannabinoid system and the immune response, and on how use of cannabis may alter one’s susceptibility to or prognosis of infections with TB and similar microbial pathogens. However, the bactericidal effect of cannabinoids is certainly of interest to researchers, and as the issue of drug-resistant bacteria becomes ever more relevant, cannabis is sure to have a part to play in their control and management.
- Disclaimer:This article is not a substitute for professional medical advice, diagnosis, or treatment. Always consult with your doctor or other licensed medical professional. Do not delay seeking medical advice or disregard medical advice due to something you have read on this website.


I have been a canabis smoker for 8 years now….i have also been a victim of TB in the course of the 8years ..but still was a cig smoker in the time of infection…..though my consistent use of canabis has been ever helpfull i dont regret it …actually i appreciate it alot for my breathing has always been up to per since before and after infection.
I am a chemist researching anti-mycobacterial plant terpenes, do you have any journal references that I could read?
Thx!
Hi Sasha,
You are probably already familiar with the PubMed site, but that’s what we often use for research. Here’s their results for anti-mycobacterial plant terepenes: https://www.ncbi.nlm.nih.gov/pubmed/?term=anti-mycobacterial+plant+terpenes I hope you continue to enjoy the blog.
With best wishes,
Scarlet
The questions above are not seeking medical advise but only clarification.
I completely agree, been doing some research on cannabis and TB because my grandmother has just been diagnosed. I’ve been a user for over 10 years now and I want to help her so badly! Thank god the research has been shedding some light on this, definitely bringing it up with the doctor.
Hello there! Thank you for your information, it really give me a big help for my website to know a lot more about treatment .
is cannabis usuful or harmful to latent or to treat and /or active tuberculosis?
Hello Ge,
Thank you for your comment. Unfortunately, as Sensi Seeds is not a medical practice, we are not able to provide any advice relating to medical situations other than to consult your doctor or other licensed medical professional. This article, written specifically for healthcare providers who may not be aware of the many properties of cannabis, may be useful to you in talking with your doctor. You could also try to contact local medicinal cannabis support groups, if you have not already done so. In the UK, there is the United Patients Alliance (you can find them on Facebook) and in the US and EU there are many branches of NORML (google NORML followed by your area name). We hope this is helpful.
With best wishes,
Scarlet
I smoke weed a few time a year but not a lot. For some reason I can breath better after I smoking weed. I only smoke weed 1x a year or none.
Amazing post with lots of information.
Pardon me , but I did not really understand this statement: ” Thus, in instances where activation of the Th1 immune response is crucial to fighting off an infection, as is the case with tuberculosis, it would appear that avoiding the use of cannabis would be advantageous”.
My question is , is cannabis usufel or harmful to latent and /or active tberculosis? Is the cannabis oil as useful or not? Thanks for the article and any info plus you may give me.
My husband had symptomatic TB for six months before diagnosis, as did several of our friends at the time. I was tested and retested several times over and remained microbe free. As the only consistent cannabis user of the group I can only put my immunity down to the smoking of cannabis. Even the specialist was surprised that I did not contract even the latent version of the disease.
oh thankyou sir, i hope u come visit my pages on facebook
https://www.facebook.com/gmi420indonesia?fref=ts 🙂
may i shared this article on the my pages?
Of course Zacky!